By Tanveer Ahmed Khan K11-Certified Fitness Trainer | REPS India Registered Dietitian-Nutritionist | 12+ Years Clinical & Coaching Experience
Key Takeaway: A June 2026 meta-analysis in The BMJ — the largest of its kind, covering 69 randomised trials and nearly 154,000 people — found that calcium and vitamin D supplements provide little to no meaningful protection against fractures or falls in most older adults. This changes what we should be recommending for bone health, and here is what actually works instead.
The Supplement That Millions of People Are Taking — And New Research Says May Not Be Doing What They Think
Walk into any pharmacy, supermarket, or health food store, and you will find calcium and vitamin D supplements marketed as the straightforward solution to bone health, fracture prevention, and healthy ageing. Millions of people globally take these supplements daily, many based on recommendations from their doctors, and many more based on decades of public health messaging that has treated calcium supplementation as a near-universal good.
A comprehensive review published in The BMJ on June 15, 2026 — one of the largest and most rigorous investigations ever conducted on this question — fundamentally disrupts that assumption.
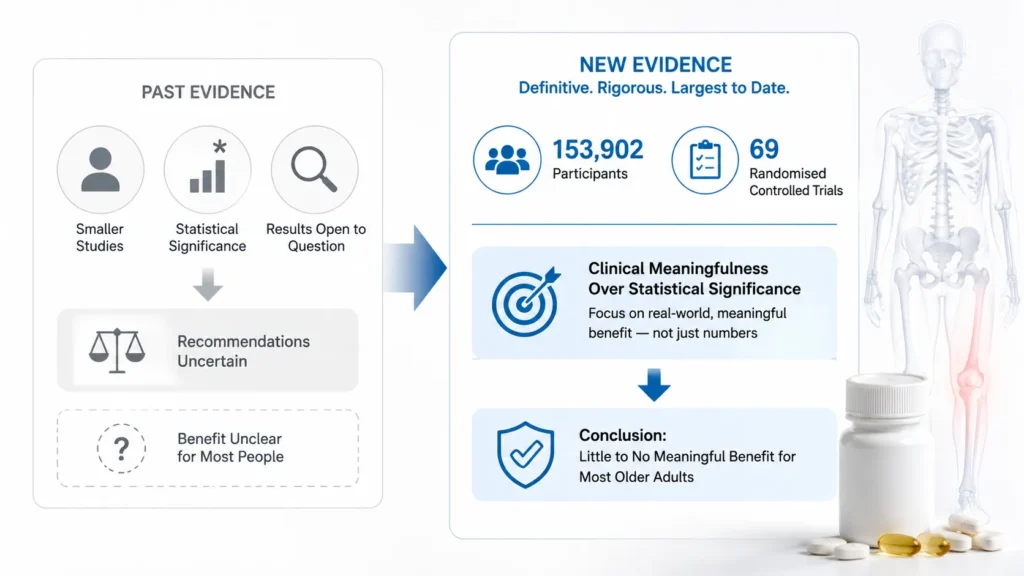
The research team, led by Olivier Massé and colleagues at a Canadian institution, analysed 69 randomised controlled trials involving 153,902 adults. Their conclusion: calcium supplements, vitamin D supplements, or the combination of both provided little to no clinically meaningful benefit in preventing fractures or falls for most older adults living independently.
This is not a small study with methodological weaknesses. This is 69 randomised controlled trials, nearly 154,000 participants, and a rigorous methodological choice that makes it more trustworthy than most prior reviews: the researchers used pre-agreed thresholds for what would constitute a clinically meaningful benefit — not merely statistical significance. This distinction matters enormously.
The Difference Between Statistical Significance and Clinical Meaningfulness
Before I explain the findings in detail, I want to make sure this methodological point lands — because it is the key to understanding why this study matters more than some previous research on the same topic.
Statistical significance simply means a result is unlikely to have occurred by chance. A supplement could show a statistically significant 1% reduction in fracture risk — technically a “real” finding — but in practice, a 1% reduction is meaningless to the individual taking the supplement. It changes nothing in their life.
Clinical meaningfulness asks a different question: Is the effect size large enough to actually matter to the patient? Is it large enough to justify the cost, the pill burden, the potential side effects?
The Massé team pre-agreed on thresholds for clinical meaningfulness before analysing their data, then asked whether calcium and vitamin D met those thresholds. The answer, across the full dataset, was no.
Specifically: calcium supplementation alone showed little to no reduction in overall fracture risk (moderate certainty evidence from 11 trials; 9,067 participants). Vitamin D alone performed similarly. The combination of both showed a slight statistical trend toward fracture reduction — but this trend did not meet the pre-agreed threshold for clinically meaningful benefit.
The researchers acknowledged that these findings may not apply to people with specific bone disorders, confirmed deficiency states, or those already receiving pharmacological treatment for osteoporosis. But for the general older adult population taking these supplements routinely as preventive measures, the evidence no longer supports the practice.
This Is Not Entirely New — But Now the Evidence Is Definitive
I want to be transparent: this is not the first time calcium and vitamin D supplementation has come under scrutiny. The US Preventive Services Task Force has previously recommended against routine vitamin D supplementation for fracture and fall prevention. Prior meta-analyses had begun raising similar questions.
What makes the June 2026 BMJ publication different is the scale — 153,902 participants across 69 trials — and the methodological rigour. Previous reviews that appeared to show benefit often used statistical significance as their criterion, which, as I described above, inflates the practical importance of small effects. This review corrected that error systematically.
As someone who has been advising clients on supplementation for over 12 years, I will admit this finding prompted me to revisit the recommendations I give. And upon reflection, it reinforces what experience had already been suggesting: the relationship between nutritional supplements and disease prevention is rarely as simple as taking a pill.
What Is Actually Happening to Bone Health as We Age?
To understand why calcium supplementation may not work as advertised, it helps to understand the biology of bone ageing — because it is more complex than the “calcium in, strong bones out” model that supplement marketing implies.
Bone is not a static structure. It is living tissue that is continuously being broken down by cells called osteoclasts and rebuilt by cells called osteoblasts. This process of bone remodelling is regulated by a complex network of hormones, mechanical signals, and nutritional inputs.
As we age, several things happen:
Osteoclast activity begins to outpace osteoblast activity. The breakdown of bone becomes faster than the rebuilding. This is the fundamental mechanism of age-related bone density loss.
Oestrogen decline in women accelerates this imbalance. Oestrogen is a key regulator of osteoclast activity — it suppresses excessive bone breakdown. When oestrogen levels fall at menopause, osteoclast activity increases dramatically, which is why women lose bone density faster than men in the years immediately following menopause.
Protein intake becomes increasingly important. Collagen is the structural scaffold of bone — approximately 30% of bone mass by weight. Adequate dietary protein is required to maintain collagen synthesis. Many older adults are protein deficient, and this contributes significantly to bone fragility.
Mechanical loading is the primary stimulus for bone formation. This is the critical point. Osteoblasts — the bone-building cells — are stimulated primarily by mechanical stress. When bones are loaded with weight and force, they respond by building more matrix. When they are not loaded — when the body is sedentary — bone formation declines regardless of calcium intake.
This last point explains a great deal about why calcium supplementation alone fails to prevent fractures. You can supply all the calcium you want, but without the mechanical signal to use that calcium for bone construction, the body does not build bone in the way the supplement marketing suggests.
What the Research Says Actually Works for Bone Health
1. Resistance training and weight-bearing exercise
This is the single most evidence-supported intervention for bone health across the lifespan. And with the June 2026 JACC study simultaneously demonstrating that resistance training reduces heart attack risk in women by 44%, the case for making strength training the centrepiece of any bone health strategy has never been stronger.
When you perform weight-bearing exercise — walking, jogging, dancing, climbing stairs — and resistance exercise — lifting weights, resistance band training, bodyweight exercises — bones experience compressive and tensile forces that directly stimulate osteoblasts to lay down new bone matrix.
Studies consistently show that regular resistance training increases bone mineral density at the hip and spine — the two sites where fractures in older adults are most dangerous and most likely to be fatal. The effect is greatest when started earlier in life but remains meaningful even when started at 60, 70, or beyond.
In my practice, I have worked with women in their 50s and 60s who were told by their doctors to “take calcium and vitamin D” for osteoporosis risk. My approach is different: I design a structured resistance training programme specifically targeting the lower spine, hip, and forearm — the fracture-vulnerable sites — and track their bone density markers over time. The results consistently show improvements that supplementation alone was never delivering.
2. Adequate dietary protein
As I noted above, collagen is the structural scaffold of bone. Adequate protein intake — particularly from a variety of sources that provide complete amino acid profiles — supports the maintenance of this scaffold.
For older adults concerned about bone health, I recommend 1.2 to 1.6 grams of protein per kilogram of body weight daily, with an emphasis on high-leucine sources that stimulate muscle protein synthesis: eggs, dairy, legumes combined with whole grains, and fish. Leucine is the primary amino acid that triggers the mTOR pathway — the cellular signalling cascade that activates both muscle and bone building.
3. Vitamin K2 — the overlooked co-factor
Here is a nutritional detail that does not receive nearly enough attention in mainstream bone health discussions, and one I consider essential clinical knowledge.
Vitamin K2 (specifically the MK-7 form) is required to activate osteocalcin — the protein responsible for binding calcium to the bone matrix and incorporating it into bone structure. Without adequate vitamin K2, calcium in the bloodstream cannot be effectively directed to bone.
This may partially explain why calcium supplementation often fails: if vitamin K2 is deficient, the calcium cannot be properly incorporated into bone tissue regardless of how much is being consumed. The calcium may instead deposit in soft tissues and arteries — a potential cardiovascular risk that some researchers have raised concerns about.
Rich food sources of vitamin K2 include fermented foods (natto is the richest known source), hard cheeses, egg yolks, and some fermented dairy products. For clients with confirmed low bone density, I often recommend a targeted K2 supplement alongside food-based sources.
4. Sun exposure and genuine vitamin D sufficiency
Let me be clear: this does not mean vitamin D is unimportant. Vitamin D deficiency is genuinely harmful and affects a substantial proportion of the global population, particularly in regions with limited sunlight exposure.
The issue the June 2026 BMJ review raises is with supplementation as a universal preventive measure for fractures in people who may not be deficient. If your vitamin D level is already adequate, supplementing further does not appear to add meaningful fracture protection.
The primary recommendation I give is to first assess vitamin D status through a blood test (25-hydroxyvitamin D), then address deficiency through a combination of sensible sun exposure (15–20 minutes of midday sun on exposed skin, without sunscreen, three to four times per week) and targeted supplementation only for confirmed deficiency states.
Who Should Still Consider Calcium and Vitamin D Supplements?
This is an important nuance, and I want to address it directly.
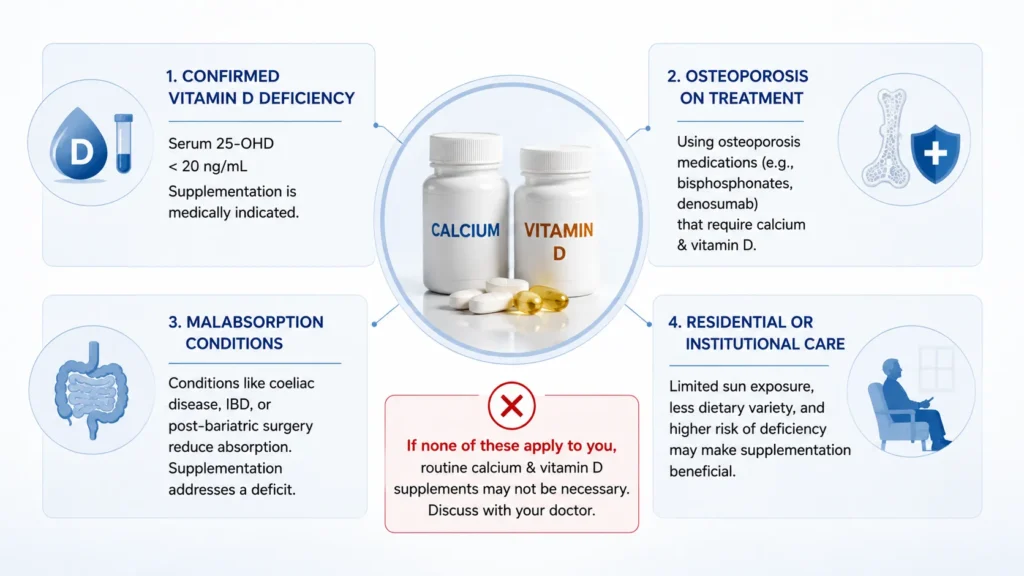
The BMJ meta-analysis findings apply to the general older adult population taking supplements as routine fracture prevention. There are specific populations for whom supplementation remains clinically appropriate:
Confirmed vitamin D deficiency (serum 25-OHD below 20 ng/mL). In this case, supplementation to correct the deficiency is medically indicated and beneficial.
Diagnosed osteoporosis being treated pharmacologically. The drugs used for osteoporosis (bisphosphonates like alendronate, denosumab, etc.) are often combined with calcium and vitamin D because the medications work through mechanisms that require these nutrients. In this clinical context, supplementation has a different rationale.
Malabsorption conditions. People with conditions like coeliac disease, inflammatory bowel disease, or post-bariatric surgery have reduced ability to absorb calcium and vitamin D from food. Supplementation in this context addresses a genuine absorption deficit.
Older adults in residential or institutional care. Some sub-analyses within the BMJ review did suggest potential benefit for this specific population — likely because institutionalised older adults may have limited sun exposure, less dietary variety, and more profound underlying deficiencies.
If you fall into none of these categories and are taking calcium and vitamin D supplements primarily as routine fracture prevention, the June 2026 evidence suggests a conversation with your doctor about whether to continue is warranted.
The Practical Bone Health Protocol I Use With Clients
Based on 12 years of working with clients across a wide range of ages and bone health profiles, here is the framework I apply:
Step 1: Test, don’t guess. Before recommending any supplement, I recommend a full baseline assessment including serum 25-OH vitamin D, a DEXA scan for bone mineral density if age and risk factors warrant it, and dietary analysis for protein, calcium-rich food sources, and vitamin K2 intake.
Step 2: Build a resistance training practice. Two sessions per week of weight-bearing resistance exercise targeting the major muscle groups, with specific attention to hip, spine, and lower body loading. This is the single most evidence-supported intervention for bone density.
Step 3: Optimise dietary calcium, not supplemental. The research does not suggest that calcium is unimportant — it suggests that supplemental calcium may not deliver the benefit that food-based calcium does. I prioritise dietary calcium from whole food sources: dairy products (yoghurt, paneer, milk), calcium-set tofu, sesame seeds, ragi (finger millet — one of the richest plant-based calcium sources at 344 mg per 100g), and dark leafy greens.
Step 4: Address vitamin K2. Include fermented foods, egg yolks, and aged hard cheeses regularly. Consider a targeted K2 supplement if dietary sources are limited.
Step 5: Supplement strategically, not universally. Only supplement vitamin D if blood testing confirms deficiency. Only supplement calcium if dietary intake is genuinely inadequate and non-supplemental approaches have been optimised.
The Takeaway
The June 2026 BMJ meta-analysis, covering 153,902 people across 69 randomised trials, delivers a clear message that runs counter to decades of supplement marketing: for most older adults, routine calcium and vitamin D supplementation does not meaningfully prevent fractures or falls.
This does not mean calcium and vitamin D are unimportant. It means that a pill is a poor substitute for the actual drivers of bone health: mechanical loading through resistance exercise, adequate dietary protein and calcium from whole foods, vitamin K2 co-factors, and sensible sun exposure.
In over a decade of practice, I have never seen a supplement produce the bone health outcomes that a well-designed resistance training programme, paired with a nutrient-dense whole-food diet, consistently delivers. The June 2026 research confirms what clinical experience had already been suggesting.
Invest in your bone health through movement and real food first. Use supplements to address specific, confirmed deficiencies — not as a replacement for the harder, more powerful, more proven interventions.
Scientific References
- Massé, O. et al. (June 15, 2026). Calcium, vitamin D, or combined supplementation to prevent fractures and falls: systematic review and meta-analysis. BMJ, 393: e088050. https://doi.org/10.1136/bmj-2025-088050
- ScienceDaily / BMJ Group. (June 15, 2026). Millions take calcium and vitamin D for stronger bones. A major review finds little benefit. https://www.sciencedaily.com/releases/2026/06/260614011852.htm
- Medical News Today. (June 26, 2026). Vitamin D, calcium may not be as helpful for strong bones as thought. https://www.medicalnewstoday.com/articles/calcium-vitamin-d-supplements-little-no-benefit-aging-bones-fractures-falls-study
- The Conversation. (June 23, 2026). Vitamin D and calcium supplements may not protect against bone fractures, large new study suggests. https://theconversation.com/vitamin-d-and-calcium-supplements-may-not-protect-against-bone-fractures-large-new-study-suggests-285425
- Medicalxpress. (May 20, 2026). Calcium and vitamin D supplements offer little to no meaningful benefit on fracture, fall prevention, review concludes. https://medicalxpress.com/news/2026-05-calcium-vitamin-d-supplements-meaningful.html